Senior citizens need help and encouragement to remain active as they age in their own communities. Given the choice, that’s what most would prefer. The smart city can provide the digital infrastructure for them to find and tailor the local neighbourhood information they need to achieve this.
Our research shows senior citizens want to pursue active ageing as a positive experience. This depends on them being able to stay healthy, participate in their community and feel secure.
Most city planning efforts to encourage active ageing are siloed and fragmented. Older people are too often shut away in retirement villages or nursing homes rather than living in the community. Current approaches are often based on traditional deficit models of focusing on older people’s declining health.
Another issue is that senior citizens are treated as receivers of solutions instead of creators. To achieve real benefits it’s essential to involve them in developing the solutions.
Working towards age-friendly cities
To counter a rise in urban ageism, the World Health Organisation (WHO) has been promoting age-friendly cities for nearly 15 years. Its age-friendly framework includes these goals:
Smart city approaches can make urban neighbourhoods more age-friendly. One way technology and better design do this is to improve access to the sort of information older Australians need – on the walkability of neighbourhoods, for example.
It’s useful for older people to be able to find out which walking routes have shade and places to stop and rest. Shutterstock
Our research has considered three factors in ensuring smart city solutions involve older Australians and work for them.
Replace ageism with agency
Government efforts have focused on increasing life expectancy rather than improving quality of life and independence. Ignoring quality of life leads to the perception of an ageing population as a burden to be looked after.
It would be better to bring about changes that improve older people’s health so they can participate in neighbourhood activities. Social interaction is a source of meaning and identity.
Active participation by older adults using digital devices can give them agency in their lives and reduce the risk of isolation. Bloomberg reports older adults have become empowered using technology to overcome social isolation during the COVID-19 pandemic.
Connect to smart city data
Cities are about infrastructure. Senior citizens need to have access to information about this infrastructure to be motivated to spend time in their neighbourhood and reduce their risk of isolation.
Growing numbers of active ageing seniors are “connected” every day using mobile phones to interact with smart city services. Many have wearable devices like smart watches that help monitor and manage their health and physical activity.
These personal devices can also be used to better connect older adults to public data about urban environments. For example, imagine an age-friendly smart city “layer” linked to a smart watch, to highlight facilities such as public toilets, water fountains and shaded rest stops along exercise routes.
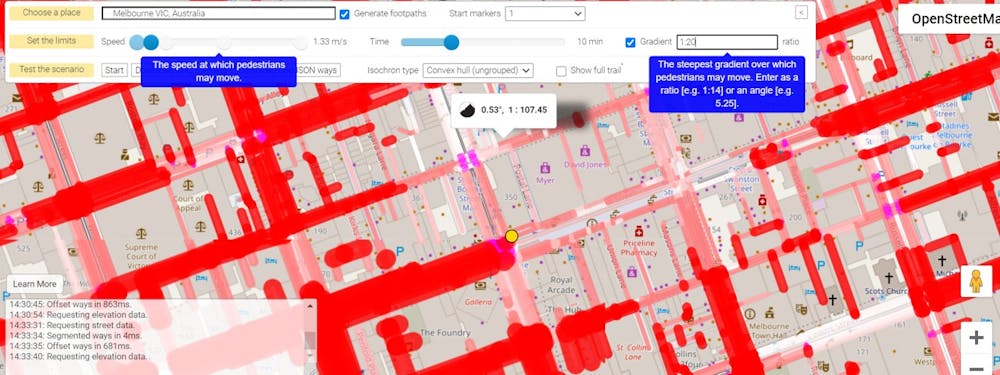
Access Map Seattle is an example of an age-friendly, interactive, smart city map that shows the steepness of pedestrian footpaths and raised kerbs. The National Public Toilet Map, created by the Australian Department of Health and Ageing, and Barcelona’s smartappcity are among other mobile apps integrating city services and urban plans.
The rise of “urban observatories” has increased the gathering and analysing of complex city-related data. These data make it possible to build a digital city layer.
PedCatch is an app that combines animated pedestrian accessibility modelling, topographical mapping and crowd-sourced geospatial data. Marcus White, Swinburne University, Author provided
This information then helps us understand and improve the liveability of neighbourhoods for older adults. The data can be used for more proactive policy and city planning.
We need to start asking senior citizens questions like “How would you like to access this data?” and “What would you like the digital layer to tell you?” Their goals and needs must drive the information provided.
It’s not just a matter of deciding what specific data older adults want to get via their devices. They should also be able to contribute directly to the data. For example, using a mobile app they could audit their neighbourhood to identify features that help or hinder walkability.
To create truly age-friendly smart cities, it is important for older people to be co-designers of the digital layer. The co-design includes deciding both the types of data available and how the data can be usefully presented. We also need to understand what mobile apps could use the data.
If we know what information within the digital city layer motivates older adults to participate more actively in their neighbourhoods, we can plan more age-friendly cities.
Through connecting infrastructures and citizen-led approaches, we can achieve social participation and inclusion of citizens regardless of their age and recognising diversity and equity. We will create places where they feel capable and safe across a range of activities. Redesigning age-friendly and smart communities directly and collaboratively with those affected can enable them to achieve the quality of life they desire.
The coronavirus has been escaping with distressing frequency from quarantine hotels, threatening serious outbreaks. To make things worse, multiple variants of the virus, possibly more infectious and deadly, have recently been detected. This accentuates the need for robust hotel quarantine, especially in countries like Australia that have controlled community transmission.
While the hotel quarantine system has received wide attention, relatively few people have had the opportunity to experience and observe it first hand. Even fewer have been able to compare with other regions handling similar challenges. I happen to have needed to travel overseas and thus experienced quarantine in several places over the past months.
Based on my experience as an academic in architecture, I share some thoughts and observations here on how the design or redesign of buildings, infrastructure and cities can help people overcome the health challenges created by COVID-19.
Our buildings and cities were not designed to handle such extraordinary situations as this pandemic. One consequence is their design has often made the need to touch surfaces unavoidable.
Some of the most frequently touched surfaces in buildings are the buttons in lifts. In some buildings in China, plastic wrap is used to cover the buttons and a sticker showing the time and date of last disinfection is attached nearby. Other buildings provide tissues for people to use as disposable finger covers.
In quarantine hotels, this procedure is even more carefully managed. Staff help guests by pressing the button. This small touch area needs frequent cleaning, which calls for extra human resources.
Various strategies used in public lifts. Above left, in Melbourne; above right and below left, in Kunming; below right, in Guangzhou. Photos: Mengbi Li (top row and bottom left), Fei Zhou (bottom right)
At Baiyunshan airport in Guangzhou, I used a lift with touch-free buttons. The keypad had infrared sensors installed next to the usual button. With just a wave of their finger over the touch-free button, users can select their destination.
A lift with infrared sensors at Baiyunshan airport in Guangzhou. Photo: Xiao Xu
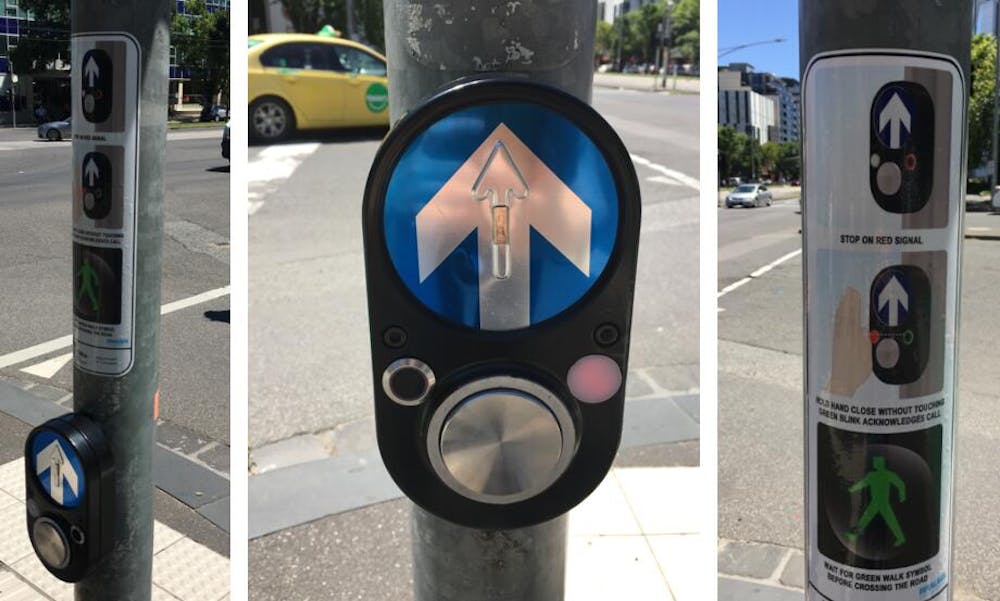
This technology is not out of our reach. In response to the pandemic, authorities in Melbourne and Sydney have trialled touch-free buttons using infrared technology at pedestrian crossings.
A pedestrian crossing signal with an infrared sensor in Melbourne. Photo: Mengbi Li, Author provided
One concern about touch-free buttons is the challenge they present to the visually impaired. Currently, a push-button is placed next to the infrared sensor. An alternative for people who need assistance would be to use gesture or voice commands. Other concerns include reliability and vandal-proofing.
Another sensitive touch spot is the toilet. The airport toilets I visited in Australia, China and Singapore are equipped with touch-free features to activate the flush, tap, soap dispenser and hand dryer. However, the doors and locks cannot function without touch. Touch-free sensors or foot pedals would probably help.
Alternatively, new materials or coatings like antimicrobial polymers could be applied in areas where touch is unavoidable. Of course, care must be taken to ensure the antiviral potency is both reliable and people-friendly.
A touch-free hand sanitiser dispenser in Melbourne. Photo: Mengbi Li
Interestingly, touch-free public spaces do not always rely on advanced materials or sophisticated technology. In a Melbourne quarantine hotel, I noticed several bollards with foot pedals being used as hand sanitiser dispensers. These are designed to function mechanically and require no power connections.
Instead of a simple stainless steel bollard, this dispenser could be further reimagined as an artistic sculpture integrating the building’s signage at the entrance. Elsewhere, this design could be incorporated into litter bins along the streets.
Usually, for architectural design, circulation patterns are analysed to see how people reach each space and establish the relationships between different areas. For safety purposes, exits are checked to ensure people can evacuate in a timely way. To prepare for future pandemics, these studies could add analysis of touch points in both pandemic and non-pandemic periods.
Plug-in intensive care units created from a shipping container were installed at a temporary hospital set up in Turin, northern Italy. Max Tomasinelli/Carlo Ratti Associati
From touch-free public spaces to designing for social distance and modular construction, there are still many ways the design or redesign of our buildings and cities can help to protect the public. Good design is particularly important to protect those in high-risk environments, such as workers and senior citizens in health care and aged care.
Press release from Alzheimer’s Disease International
8 October 2020
Partners Launch Dementia Innovation Readiness Index to Challenge Cities to Develop and Adopt Innovations Across the Global Dementia Community
Today, the Global Coalition on Aging (GCOA) and Alzheimer’s Disease International (ADI), in partnership with Singapore’s Lien Foundation, will present findings from the 2020 Dementia Innovation Readiness Index showing that cities have largely failed to support innovation in dementia comprehensively, though bright spots exist.
By mid-century, the number of those aged 65 or older set to double, and nearly two-thirds of the world’s population will live in urban areas, up from just over half today. The number of older people in cities is growing faster than in rural areas, according to the OECD.
Given these shifts across society, the need for local leadership to address dementia is clear, yet the Index findings suggest that cities around the world have not fully leveraged opportunities to support the development or adoption of innovations in dementia care, treatment and support and should take a leadership role in dementia innovation readiness. Rated on a 0-10 scale, the top five performing cities in the Index overall were London (8.4), Glasgow (7.8), Manchester (7.7), Amsterdam (7.5), and Vancouver (7.5). Top-performing cities tend to be in high-income countries with some level of nationalized healthcare, and a national plan in place that helps to promote innovation at the city-level.
Among the 30 cities profiled, assessments reveal that London and Glasgow lead in strategy and commitment and community support for individuals living with dementia, as local associations play a pivotal role in the formation of the national response on dementia.
“This year’s Dementia Innovation Readiness Index establishes the foundation for high impact, action-oriented initiatives to promote collective action from governments, industry, NGOs, academics and other leaders,” said Michael W. Hodin, PhD, CEO, GCOA. “Cities must rise to the challenge presented by global aging and build the capacity and opportunity to improve health outcomes for people living with dementia because they are at the forefront of innovation in their communities.”
Measured against 26 indicators and across five categories, including strategy and commitment, early detection and diagnosis, access to care, community support, and business environment, findings revealed that while leadership is present throughout the global community to meet the overwhelming demands for quality dementia care, significant gaps persist.
“The Index gives us a snapshot of how prepared some of our major cities are to embrace dementia innovation,” said Paola Barbarino, CEO, ADI. “During COVID-19 we have seen how important cities have been in managing the pandemic. With their large concentration of population, cities have an opportunity and a challenge to drive best practice. From a policy perspective, the Index provides a call to action for local and national governments to drive policies to better the lives of those affected by dementia and their loved ones.”
The Index’s main findings include:
Cities must take charge to execute against national dementia plans. Tasking ministries, agencies, civil servants, or other permanent policy bodies with implementing a plan at the local level can help to ensure dementia remains front-and-center, even as political leadership changes, and when plans are backed by adequate funding, they are a key enabler of dementia innovation.
Cities must advocate for flexible and transparent funding models enabling regions and cities to adapt national programs and frameworks to local contexts.
Cities need to know where they stand with regard to the number of people in the community living with dementia. Accurate, early diagnosis can help to ensure that people living with dementia are able to access high-quality care; that the progression of their disease is appropriately managed and monitored; and that they will be able to expediently access innovations in treatment and care as they become available.
National-level efforts to improve diagnosis rates for dementia should be aligned with the local community. One of the most common misconceptions about dementia is that it is simply a normal part of aging, and cities must be ready to deploy population-specific messaging, screening tools, and other resources that are adaptable to the diverse communities residing there.
Post-diagnostic support is a highly localized but under-addressed opportunity for cities. City stakeholders can collaborate across the medical, social, and policy fields to ensure that locally tailored post-diagnostic support is in place and that healthcare professionals and other community service providers have the knowledge and training to connect people with relevant programs.
Local governments and service providers must ensure that there is a sufficient supply of affordable and high-quality community-based care providers — including day care, respite care, and in-home care — so that people living with dementia are able to access needed resources. In areas where the care workforce is insufficient to adequately support people living with dementia, local stakeholders can help to build the workforce through training, increased access to educational and vocational services, as well as immigration, thus creating local jobs while solving for the impending care crisis.
Cities should engage and fully leverage non-profit Alzheimer’s and dementia associations as experts in the community.
Dementia-friendly principles are the tools and practices that make an organization, community, or society-at-large more accessible and livable for people with dementia, but they also enhance cities and improve quality of life for all citizens.
Cities have a role in enabling new and existing funding models for dementia research. For example, venture capital funding (through organizations like the Dementia Discovery Fund) and social impact bonds by cities can spur innovation. Such efforts will serve as a catalyst for breakthrough research and offset the perceived risk brought by slow therapeutic progress and growing investor hesitancy toward dementia.
The Index also identifies examples of leading practices – in cities large and small, developed and developing – across the five key areas of the Index, which can serve as a model for others in the global community.
“Aging and urbanization are the twin defining trends of our time,” said Radha Basu, Research Director, Lien Foundation. “As societies age and dementia becomes more common, this Index issues a clear call to city-level leaders and help cities learn from each other on how to best manage this great, global challenge to health and social care.”
Insights from the Index were informed by input from interviews and surveys with global key opinion leaders and subject matter experts (including scientists, advocates, researchers, clinicians, business leaders, and people living with dementia). As well as secondary research that was gathered from global authorities including ADI, the Organisation for Economic Co-operation and Development, the World Health Organization, and other publicly available sources.
Thirty years ago dementia was a condition less understood than it is now and assumed to be a normal part of ageing. A condition which affects the memory, it can also affect sight, hearing, balance, walking, visual and spatial understanding, navigation and tonal differentiation, and can cause hallucinations.
Today, dementia affects approximately 50 million people worldwide and is predicted to double in 20 years due to an ageing population and an increase in awareness and diagnosis. Dementia has become a global issue.
The design of the built environment can have a profound impact on how a person with dementia perceives, experiences and engages with the places and spaces in which they live. Yet much of the design guidance currently available is underpinned by research undertaken in developed countries.
Research has shown that rather than drawing upon the experiences of older people, their families and care professions, architects designing for later life are more likely to draw upon presumed needs and experiences of the older person as imagined by themselves.
This begs the question of who will lead the global challenge to ensure spaces and buildings support this increase in the prevalence of dementia while retaining all the beauty, joy and quality of life that good architecture and design can bring. https://www.youtube.com/embed/6cpWVGZWebA?wmode=transparent&start=0
Dementia design principles
Dementia design is a non-medical approach to help reduce some of the symptoms associated with dementia, such as agitation, aggression, confusion, incontinence and visual, spatial and navigational difficulties.
The international consensus on principles agrees that dementia design should incorporate the following concepts: it should compensate for disability, maximise independence and enhance self-esteem and confidence. It should also demonstrate care for staff needs, be orientating and understandable, reinforce personal identity, welcome relatives and the local community, and allow control of stimuli – for example, reducing unwanted noises associated with alarm systems.
Dementia design principles came into being in the late 1980s when the development of Confused and Disturbed Elderly (CADE) units in New South Wales, Australia, established a design brief which advocated for specific principles to support those living with dementia. Soon after, the Dementia Services Development Centre (DSDC) was established at the University of Stirling, which became influential in this field.
People with dementia have particular needs that can be addressed by good design and thoughtful buildings and environments. Lesley Palmer, Author provided
At the time, leaders in this field called on architects to consider dementia not as a disease, focusing design on spaces that support physical decline, but rather as a disability where the design focus shifts to spaces that can maintain everyday functions of people living with dementia. The importance of this juxtaposition should not be underestimated and is better understood in the context of the seismic shift that was happening in built environment legislation in the UK.
The Disability Discrimination Act of 1995 (DDA) placed an obligation on spaces to be free from discrimination – the environment being the disabling factor affecting opportunities to participate in everyday life. The new act resulted in a wholescale review of how the built environment supported – or didn’t – those with physical impairments.
Architecture and the codes which govern it were redesigned. Proponents of dementia design witnessed this and lobbied for this approach to include people living with dementia, but there has been very little progress on this issue until recently.
Dementia design today
Developments in dementia research recognise that the condition is not a natural part of ageing, but that the risk of developing it increases with age. Alcohol, smoking, cholesterol and diabetes also increase the risk of dementia, and air pollution has been also identified as impacting on brain health.
There is also a growing call for intergenerational living and dementia design principles are being integrated into age-friendly projects such as retirement living and community buildings.
For the most part this is encouraging. An age-friendly city could foster healthy and active ageing by building and maintaining that capacity across the course of people’s lives. It could support the development of healthy brain function from early years, help people maintain cognition through their later years and support cognitive decline as people age.
Green spaces are important for physical and mental well-being. Shutterstock
A public health issue
Thinking ahead and considering the complex causal factors, increased diagnosis rates and multi-disciplinary scope of dementia therapies, people living with the condition and their families would benefit from a coordinated global response in every country and across all cultures. Early proponents of dementia design advocated for dementia to be considered as a disability which required spaces that maintain function. I believe it would also be helpful to recognise dementia as a public health issue and use design to address some of the challenges this brings.
This would enable architects and planners to integrate dementia-design principles in a similar fashion to the way in which the Disability Discrimination Act supported people with physical disabilities. They could employ the tools of health impact assessment to plan places to support prevention by reducing the risk of developing some of the underlying health conditions mentioned earlier. The provision of green spaces, active travel and play, walkable neighbourhoods, improved biodiversity and air quality could all help the fight against dementia.
To fully understand the benefits, there is a pressing need for critical discussion and further research and architectural projects with briefs which challenge designers to address this important global issue.
Acknowledging more than 30 years of dementia design, Stirling University’s Dementia Services Development Centre has launched Architecture for Dementia: 2008-2020 – a unique selection of outstanding projects from across the globe. Each one has received a DSDC “Stirling gold” for dementia-friendly buildings.
If there was ever a time to celebrate evidence-based dementia design, it is now. This record will stand as a baseline for the development of the next 30 years of progress in the design of dementia-inclusive design and help improve the quality of life for millions of people around the world living with this debilitating condition.
Press release from Alzheimer’s Disease International
21 September 2020
Dementia design in built environment is 30 years behind physical disabilities movement
ADI calls on governments to embed design in their national dementia responses under the Convention on the Rights for Persons with Disabilities
Dementia design follows simple principles, is cost effective and dramatically improves enjoyment and safety of built environment for those living with dementia
Dementia design can enable people to live in their own homes and communities for as long as possible
ADI launches world’s most comprehensive report on dementia and design for World Alzheimer’s Day, 21st September 2020
21 September 2020 – Drastically improved dementia design in the built environment is needed across the globe according to Alzheimer’s Disease International (ADI), who are calling on governments and multilateral bodies to overtly recognise dementia as a disability following recommendations from the world’s most comprehensive ever report into dementia-related design, World Alzheimer Report 2020:Design, Dignity, Dementia; dementia-related design and the built environment[1].
On World Alzheimer’s Day, ADI is calling for dementia to be more overtly recognised by governments globally as a disability, including as part of national dementia plans, to help to ensure that the therapeutic benefits of good dementia design are felt by people living with dementia at home, in residential and day-care facilities, hospitals and public buildings and spaces.
Approximately 152 million people are forecast to be living with dementia by 2050, and it is already the fifth leading cause for death worldwide, yet most countries are woefully behind in terms of making the built environment accessible for those living with dementia.
Recognising dementia as a disability will help ensure that similar strides are made for dementia design as have been made over the last 30 years by the physical disability movement, such as seeing accessible lifts, ramps, safer pedestrian crossings and the like made commonplace across the globe.
ADI’s Chief Executive, Paola Barbarino, says that dementia design provides an opportunity to adapt built environments in the same way that physical disability design has led to great innovation.
“We need to apply design guidelines and principles for people living with dementia in the same way as design guidelines are provided for people living with a physical disability,” says Barbarino. “When I was in my first job, I remember people saying that accessible lifts and ramps were impossible to install in old buildings but look at it now! If we can cater for those with visible disabilities, how can we refuse to cater for those with invisible disabilities? We need to start working now, with new builds, and consider this new way of thinking at planning stage, and also look at cost effective retro-fit options for older buildings.”
Barbarino says that dementia design does not have to be a costly exercise and can be as simple as considering things like carpets and décor, the removal of hazards, reducing stimulation, clear wayfinding – measures that can reduce anxiety and agitation and improve social interactions.
“It comes down to simple things. I recall during a site inspection of a venue for a conference, the black areas on colourful carpets could look like holes in the floor, people living with dementia might walk around them as they could be worried of falling into them,” says Barbarino. “Things like mirrors on the walls can be an issue, as people with dementia can be disoriented by seeing their own reflection, especially at night. Design is effectively a non-pharmacological intervention, adding to the number of things we can do – in absence of a cure – to make the lives of those living with the condition easier and more fulfilling.”
Co-author of the report, Richard Fleming, says that dementia design is needed urgently, and our knowledge of how to do it has grown over the years.
“Our knowledge of how to design buildings that support people living with dementia has grown over the last forty years and we are now in a position to be more proactive in implementing it in practice,” says Fleming. “The rising number of people living with dementia requires that their needs are considered at the beginning of every building project that is likely to be used by elderly people. Dementia design should never be an afterthought.”
“We need more architects and designers who are switched on to the challenges of designing for people living with dementia. This means that they should be introduced to them in their training when they are looking for areas that inspire them,” continues Fleming. “Designing for people living with dementia should be made an attractive option in the curriculum of every school of architecture and design.”
In the report, Kate Swaffer, Chair, Co-Founder and CEO of ADI’s partner Dementia Alliance International, says that the link between disability and environment is clear.
“The environment’s influence in creating disability or in increasing it has been well established and is seen as integral to the definition of disability,” says Swaffer. “If the environment changes, then the experience of someone living with a disability will also change.
“People with physical disabilities have made major progress as substantial, influential members of society, borne out of society’s response to changes in the built environment becoming the norm in many countries” continues Swaffer. “Yet people with dementia are still being left behind, not only in terms of health and social care but in terms of recognition of dementia as a condition causing disability. It is vital that planners, designers and architects embrace dementia-related design at the outset and include people living with dementia in the whole design process”
Covid-19 has disproportionately impacted people with dementia, with around a quarter of virus deaths in certain countries being those of people with dementia. Care facilities, where many people with dementia live, have been hard hit when exposed to the virus.
“Covid-19 restrictions implemented to protect residents in long term care may have resulted in interventions that could have accelerated physical and cognitive decline or indirectly contributed to the deaths of some residents,” says Barbarino. “Better design could have absolutely helped to minimise the spread of the virus in care facilities. Dementia design needs to be a crucial part of how countries rebuild following Covid-19.”
Recognising dementia as a disability is one of several recommendations from the World Alzheimer Report 2020, alongside the recommendation to incorporate dementia-related design into national dementia plans in response to the WHO Global action plan on the public health response to dementia 2017-2025[2].
“The first target in the WHO plan is for 75 percent of the Member States to have developed or updated national policies, strategies, plans or frameworks for dementia by 2025,” says Barbarino. “Presently, only 30 Member State countries out of 146 have met this goal. The analysis of these plans available through the ADI website shows that only about 25 percent of these currently include designing for people with dementia.”
Australia, England and Scotland are global leaders in dementia-related design leading the way in translating existing research into practice. Barbarino says that these are among many great examples of existing efforts to develop dementia-friendly design, pointing to the likes of Swedish furniture giant IKEA.
“In 2019, IKEA partnered with a construction company to launch flat pack housing for people living with dementia. The homes feature key elements of dementia design, including mirrorless bathrooms, old-fashioned appliances, traditional cupboard handles in kitchens, simply adapted bathrooms and importantly dementia-friendly outdoor spaces and gardens,” says Barbarino. “Their focus has been to encourage accessibility and engagement with activities that promoted socialisation and wellbeing. With over 100 simple adaptations – many dementia specific – this is an innovative new model for living independently at home for longer.”
Barbarino says that it just one such example of how dementia design can be adopted, but that ultimately it comes back to having strong national planning for the disease.
“We cannot stress enough how important it is for countries to develop and implement national dementia plans, and to include dementia-friendly design into these plans,” says Barbarino. “Design considerations can make a world of difference for people living with dementia, helping them to live with dignity and respect.”
The principles of dementia design include:
Unobtrusively reducing risks: Minimise risk factors such as steps and ensure safety features are as unobtrusive as possible.
Providing a human scale: The scale of buildings can impact the behaviour of people with dementia, so provide a human scale to minimise intimidating features.
Allowing people to see and be seen: The provision of an easily understood environment will help to minimise confusion. A literal line of sight should be clear for both residents, and staff.
Reducing unhelpful stimulation: Environments should be designed to minimise exposure to stimuli that are unhelpful, such as unnecessary or competing noises and the sight of unnecessary signs, posters, spaces and clutter.
Optimise helpful stimulation: Enabling the person living with dementia to see, hear and smell things that give them cues about where they are and what they can do, can help minimise their confusion and uncertainty.
Support movement and engagement: Providing a well-defined pathway of movement, free of obstacles, can support engagement with people and opportunities.
Create a familiar place: The use of familiar building design, furniture, fittings and colours affords people with dementia an opportunity to maintain their competence.
Provide opportunities to be alone or with others: A variety of spaces, some for quiet conversation and some for larger groups, as well as spaces where people can be by themselves, gives people with dementia a choice to how they spend their time.
Link to the community: The more an environment enables visitors to drop in easily and enjoy being in places that encourage interaction, the more the sense of identity that comes from spending time with loved ones and others is reinforced.
Design in response to vision for way of life: The way of life offered needs to be clearly stated and the building designed both to support it and to make it evident to the residents and staff.
“As the number of people living with dementia rise, and young onset dementia is increasingly an issue, we need to build a world for people living with dementia, one that they and their families can all be proud of.”
World Alzheimer’s Month is the international campaign every September to raise awareness and challenge the stigma that surrounds dementia. September 2020 will mark the 9th World Alzheimer’s Month. The campaign was launched in 2012: World Alzheimer’s Day is on 21 September each year. For more information, please visit: https://www.alz.co.uk/world-alzheimers-month
About Alzheimer’s Disease International (ADI)
ADI is the international federation of 102 Alzheimer associations and federations around the world, in official relations with the World Health Organization. ADI’s vision is prevention, care and inclusion today, and cure tomorrow. ADI believes that the key to winning the fight against dementia lies in a unique combination of global solutions and local knowledge. ADI works locally, by empowering Alzheimer associations to promote and offer care and support for persons with dementia and their care partners, while working globally to focus attention on dementia and campaign for policy change. For more information, please visit www.alz.co.uk
Appendix:
Design, Dignity, Dementia: World Alzheimer Report 2020 will be launched by webinar on Monday 21 September 13:00 BST (London). The webinar will be hosted by ADI’s Chief Executive Paola Barbarino and will feature key expert speakers. Sign up here.
Report recommendations:
ADI will facilitate discussions on the development and adoption of a common set of design principles that will be used to structure the exploration of designing well for people living with dementia and the formulation of future recommendations.
A call for more overt and considered inclusion of dementia related design as a non-pharmacological intervention, to be included in national dementia plans, in response to the WHO Global action plan on the public health response to dementia 2017–2025
ADI, alongside partner Dementia Alliance International, and other advocacy groups, will work to give prominence to the arguments contained in the Convention on the Rights of Persons with Disabilities (CRPD) for the recognition of dementia as a disability and the consequent need to apply design guidelines for people living with dementia in the same way as design guidelines are provided for people living with a physical disability.
A call to all educators about the need to include designing for people living with dementia in the curricula of schools of architecture and design.
Encourage health economists to engage with the field of designing for people living with dementia to clearly establish the cost benefit of investment in dementia related design translating to savings in health and care costs by facilitating people to live in their own homes and their communities for as long as possible
ADI will encourage governments and academic institutions to engage researchers to translate knowledge on designing for people living with dementia. This knowledge, often gained in high income countries, can support and service development in low- and middle- income countries.
ADI will encourage National Dementia Associations to better inform themselves about the available knowledge on designing for people living with dementia, consider its relevance to their contexts and priorities, and advocate for relevant knowledge to be implemented by planners, designers, architects, care operators and developers.
ADI will encourage governments and the international community to proactively engage designers, architects, developers, operators and innovators, in the construction and IT sectors, in designing for people living with dementia.
[1] FLEMING, R., ZEISEL, J. & BENNETT, K. 2020. World Alzheimer’s Report 2020: Design Dignity Dementia, Case Studies. London, England: Alzheimer’s Disease International.
[2] Global action plan on the public health response to dementia 2017–2025. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Why are so many aged care residents and staff becoming infected with COVID-19? New research suggests poor ventilation may be one of the factors. RMIT researchers are finding levels of carbon dioxide in some nursing homes that are more than three times the recommended level, which points to poor ventilation.
An examination of the design of Newmarch in Sydney and St Basil’s in Melbourne shows residents’ rooms are arranged on both sides of a wide central corridor.
The corridors need to be wide enough for beds to be wheeled in and out of rooms, but this means they enclose a large volume of air. Windows in the residents’ rooms only indirectly ventilate this large interior space. In addition, the wide corridors encourage socialising.
If the windows to residents’ rooms are shut or nearly shut in winter, these buildings are likely to have very low levels of ventilation, which may contribute to the spread of COVID-19. If anyone in the building is infected, the risk of cross-infection may be significant even if personal protective equipment protocols are followed and surfaces are cleaned regularly.
Why does ventilation matter?
Scientists now suspect the virus that causes COVID-19 can be transmitted as an aerosol as well as by droplets. Airborne transmission means poor ventilation is likely to contribute to infections.
A recent article in the journal Nature outlines the state of research:
Converging lines of evidence indicate that SARS-CoV-2, the coronavirus responsible for the COVID-19 pandemic, can pass from person to person in tiny droplets called aerosols that waft through the air and accumulate over time. After months of debate about whether people can transmit the virus through exhaled air, there is growing concern among scientists about this transmission route.
Under the National Construction Code (NCC), a building can be either “naturally ventilated” or “mechanically ventilated”.
Natural ventilation requires only that ventilation openings, usually the openable portion of windows, must achieve a set percentage of the floor area. It does not require windows to be open, or even mandate the minimum openable area, or any other measures that would ensure effective ventilation. Air quality tests are not required before or after occupation for a naturally ventilated building.
Nearly all aged care homes are designed to be naturally ventilated with openable windows to each room. In winter most windows are shut to keep residents warm and reduce drafts. This reduces heating costs, so operators have a possible incentive to keep ventilation rates down.
From inspection, many areas of typical nursing homes, including corridors and large common spaces, are not directly ventilated or are very poorly ventilated. The odour sometimes associated with nursing homes, which is a concern for residents and their visitors, is probably linked to poor ventilation.
Carbon dioxide levels sound a warning
Carbon dioxide levels in a building are a close proxy for the effectiveness of ventilation because people breathe out CO₂. The National Construction Code mandates CO₂ levels of less than 850 parts per million (ppm) in the air inside a building averaged over eight hours. A well-ventilated room will be 800ppm or less – 600ppm is regarded as a best practice target. Outside air is just over 400ppm
An RMIT team led by Professor Priya Rajagopalan is researching air quality in Victorian aged care homes. He has provided preliminary data showing peaks of up to 2,000ppm in common areas of some aged care homes.
This figure indicates very poor ventilation. It’s more than twice the maximum permitted by the building code and more than three times the level of best practice.
Good ventilation has been associated with reduced transmission of pathogens. In 2019, researchers in Taiwan linked a tuberculosis outbreak at a Taipei University with internal CO₂ levels of 3,000ppm. Improving ventilation to reduce CO₂ to 600ppm stopped the outbreak.
Nursing home operators can take simple steps to achieve adequate ventilation. An air quality detector that can reliably measure CO₂ levels costs about A$200.
If levels in an area are significantly above 600ppm over five to ten minutes, there would be a strong case to improve ventilation. At levels over 1,000ppm the need to improve ventilation would be urgent.
Most nursing homes are heated by reverse-cycle split-system air conditioners or warm air heating systems. The vast majority of these units do not introduce fresh air into the spaces they serve.
The first step should be to open windows as much as possible – even though this may make maintaining a comfortable temperature more difficult.
Creating a flow of warmed and filtered fresh air from central corridor spaces into rooms and out through windows would be ideal, but would probably require investment in mechanical ventilation.
Temporary solutions could include:
industrial heating fans and flexible ventilation duct from an open window discharging into the central corridor spaces
radiant heaters in rooms, instead of recirculating heat pump air conditioners, and windows opened far enough to lower CO₂ levels consistently below 850ppm in rooms and corridors.
The same type of advice applies to any naturally ventilated buildings, including schools, restaurants, pubs, clubs and small shops. The operators of these venues should ensure ventilation is good and be aware that many air-conditioning and heating units do not introduce fresh air.
People walking into venues might want to turn around and walk out if their nose tells them ventilation is inadequate. We have a highly developed sense of smell for many reasons, and avoiding badly ventilated spaces is one of them.